The day the colon stops cooperating
If small bowel obstruction is the frantic traffic jam of the gut, large bowel obstruction is the motorway shutdown, slower to declare itself, but far more catastrophic when it does.
The colon, proud custodian of our digestive leftovers, is designed to move content calmly toward the exit. But when something blocks it, a tumour, a twisted loop, a stubborn diverticular stricture, the colon responds with dignified resistance… at first.
Then things get serious. Gas accumulates, the bowel dilates, the wall thins, and suddenly you have a surgical crisis brewing behind an often deceptively calm abdomen.
Causes: the usual suspects, with an obvious winner
Unlike the small bowel, where adhesions run the show, large bowel obstruction has a clear champion: colorectal cancer.
If an adult over 50 presents with LBO, assume cancer until proven otherwise.
Other causes include:
| Cause | Notes |
| Colorectal cancer | Far and away the most common cause. |
| Volvulus | Sigmoid and caecal loops twisting like frustrated pretzels. |
| Diverticular strictures | Scarring from chronic inflammation. |
| Faecal impaction | The great masquerader, especially in the elderly. |
| Inflammatory strictures | Crohn’s disease and, less commonly, ischaemic colitis. |
But never forget the golden rule: in adults, obstruction until proven otherwise = malignancy until proven otherwise.
The physiology, pressure, stretch, and impending doom
The colon is widest at the caecum. That means it is also the weakest point, the place most likely to perforate when pressure rises.
This is why LBO is so dangerous:
- The upstream colon fills with gas and faeces.
- Intracolonic pressure increases.
- Blood flow to the bowel wall decreases.
- The lumen thins, the mucosa suffers, and bacterial translocation increases.
Once pressure exceeds about 80 mmHg, the caecum may perforate. And when it does, you get faecal peritonitis, the kind of emergency surgeons never forget and patients rarely survive.
Symptoms: the grand presentation
Large bowel obstruction announces itself with regal clarity:
- Abdominal distension: dramatic, progressive, unmistakable.
- Colicky abdominal pain, often lower or central.
- Absolute constipation: no stool, no gas.
- Late vomiting: unlike SBO, vomiting arrives fashionably late.
Patients often describe feeling “full,” “bloated,” or “unable to pass anything at all.” Some can pinpoint the exact moment the bowel simply stopped cooperating.
On examination:
- Abdomen is distended, sometimes with visible loops.
- Bowel sounds may be high-pitched or absent.
- Digital rectal exam may reveal an empty rectum, a hard stool, or, occasionally, a palpable tumour.
Red flags: the signs you’re already in trouble
These features suggest strangulation or impending perforation:
- Fever
- Tachycardia
- Guarding or peritonism
- Leukocytosis
- Raised lactate
- Localised right lower quadrant pain (danger to the caecum)
Delay here is deadly.
Diagnosis: the radiology that never lies
Clinical suspicion is the beginning, but imaging seals the deal.
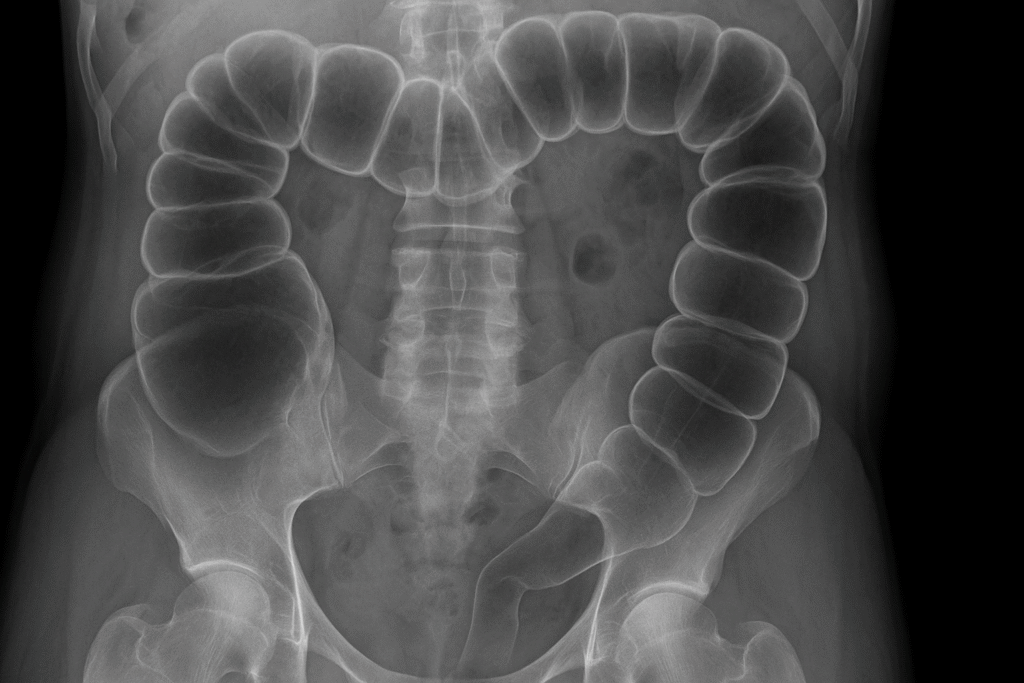
1. Plain abdominal X-ray
The humble AXR still has value:
- Peripheral dilated bowel loops (colon hugs the edges).
- Haustra visible (unlike small bowel valvulae).
- Distended caecum (>9 cm is worrying).
- Coffee-bean sign → sigmoid volvulus.
2. CT scan with contrast, the modern gold standard
CT doesn’t just diagnose; it gives answers:
- Shows the transition point.
- Distinguishes mechanical vs pseudo-obstruction.
- Identifies malignancy, volvulus, ischaemia, or perforation.
- Provides surgical roadmaps.
3. Contrast enema
Still used in volvulus, may both diagnose and untwist a sigmoid loop.
The types, simple, closed-loop, or strangulated
Like small bowel obstruction, LBO has three personalities:
| Type | Description |
| Simple obstruction | Blockage but blood supply intact. |
| Closed-loop obstruction | Blocked at two points (e.g., volvulus) → high perforation risk. |
| Strangulated obstruction | Blood supply compromised → necrosis → perforation. |
Closed-loop and strangulation are surgical “drop everything now” emergencies.
Management: stabilise, decompress, decide, operate
Large bowel obstruction is not a “wait and see” condition. It demands a structured, urgent approach.
1. Resuscitate first
- IV fluids — dehydration and third-spacing are significant.
- Correct electrolytes.
- Insert a nasogastric tube (less crucial than in SBO but still valuable).
- Catheterise for accurate urine output monitoring.
- Broad-spectrum antibiotics if perforation or sepsis is suspected.
2. Identify the cause (quickly!)
Your treatment depends entirely on the underlying pathology.
3. Specific interventions
Colorectal cancer
- Most require urgent surgery (e.g., Hartmann’s procedure, resection with diversion, or stenting as a bridge to resection).
- Stenting is ideal for left-sided obstruction in stable patients.
Sigmoid volvulus
- Try endoscopic decompression first, it works in up to 80%.
- Then perform elective sigmoidectomy later to prevent recurrence.
Caecal volvulus
- Endoscopic reduction rarely works.
- Surgery is required, often right hemicolectomy.
Diverticular stricture
- Usually needs surgical resection; stenting is less reliable.
Fecal impaction
- The rare moment when enemas and manual disimpaction save the day.
Complications: where hesitation kills
Untreated or delayed LBO can spiral into:
- Perforation (especially caecal)
- Faecal peritonitis
- Septicaemia
- Bowel ischaemia
- Shock
- Death
Large bowel obstruction gives warnings, but not for long.
A day on the surgical take
The consultant strides in, glances at the distended abdomen, and says the one phrase that instantly raises everyone’s pulse:
“Has anyone checked the caecal diameter?”
Because that number, often 9, 10, 11 cm, determines whether you still have time… or whether you’re already too late.
Within an hour, radiology confirms the obstruction, anaesthetics is preparing the theatre list, and general surgery is sharpening its collective knives.
LBO doesn’t give you gentle teaching moments, it gives you deadlines.
Clinical pearls
- Colon cancer = #1 cause of LBO. Always think malignancy.
- Peripheral gas on AXR → large bowel; central → small bowel.
- Caecum >9 cm = danger of perforation.
- Coffee-bean sign → sigmoid volvulus.
- Closed-loop volvulus = operate now.
- Don’t delay CT.
- Don’t wait for vomiting, it’s a late sign.
Closing words
Large bowel obstruction is one of surgery’s great emergencies, deceptive at first glance, unforgiving when ignored, and deeply satisfying when managed well. It’s the kind of pathology that tests judgement more than dexterity.
The colon is patient… until it isn’t.
And when it finally rebels, the window to save it is brutally small.
So, respect the distended abdomen.
Respect the silent peritoneum.
And never, ever ignore a caecum flirting with double digits.
Because once the colon says “absolutely not,” your job is to act, not admire.