The groin: small region, big problems
Few areas of the body punch above their weight like the groin.
It’s a crossroad of vessels, nerves, muscles, and just enough anatomical compromise to let abdominal contents slip through when the stars misalign.
This is where inguinal, femoral, and obturator hernias live, argue, and confuse medical students.
It’s also where surgeons earn their reputation, and occasionally lose their temper.
But fear not. Once you understand the anatomical Toblerone, everything else falls neatly into place.
The Inguinal Canal: A Toblerone With Opinions
If someone had designed the inguinal canal today, they’d be fired for structural incompetence.
It’s a triangular prism, shaped uncannily like a Toblerone bar, running obliquely above the inguinal ligament.
- One triangle marks the deep inguinal ring.
- The opposite triangle marks the superficial inguinal ring.
- Between them lies the long, mischievous prism, the canal itself.
This chocolate-bar analogy is beloved by surgeons because it’s accurate: the canal is a rigid prism with four walls, a roof, and a floor. Once you see the Toblerone, you never unsee it.
The Three Walls of the Toblerone (i.e. the canal, with a little roof):
- Anterior wall: external oblique aponeurosis
- Posterior wall: transversalis fascia (weak point!)
- Roof: arching fibres of internal oblique + transversus abdominis
- Floor: inguinal ligament
Men get the spermatic cord through this tunnel.
Women get the round ligament.
Both get hernias if the structure misbehaves.
Inguinal Hernias: the classic troublemakers
Inguinal hernias are the most common hernias in humans, especially in men, for whom the canal is a necessary evolutionary design flaw.
They come in two flavours:
1. Indirect Inguinal Hernia, the long Toblerone journey
This hernia enters through the deep ring triangle, marches through the Toblerone, and may exit via the superficial ring triangle, even descending into the scrotum.
Mechanism:
- Congenital persistence of a patent processus vaginalis
- Weakness at the deep ring
- Hernia travels lateral to the inferior epigastric vessels
Clues:
- Common in younger patients
- Appears lateral
- You can feel it touch the fingertip when you perform a cough impulse test from inside the canal (classic exam trick)
2. Direct Inguinal Hernia, the shortcut through the posterior wall
This one doesn’t bother with the Toblerone entrance.
It punches straight through the posterior wall of the canal, specifically through Hesselbach’s triangle, and bulges out medially.
Mechanism:
- Acquired weakness of the transversalis fascia
- Occurs medial to the inferior epigastric vessels
Clues:
- Common in older men
- Rarely descends into the scrotum
- On exam, the cough impulse pushes against the side of your finger, not the tip
- Often bilateral
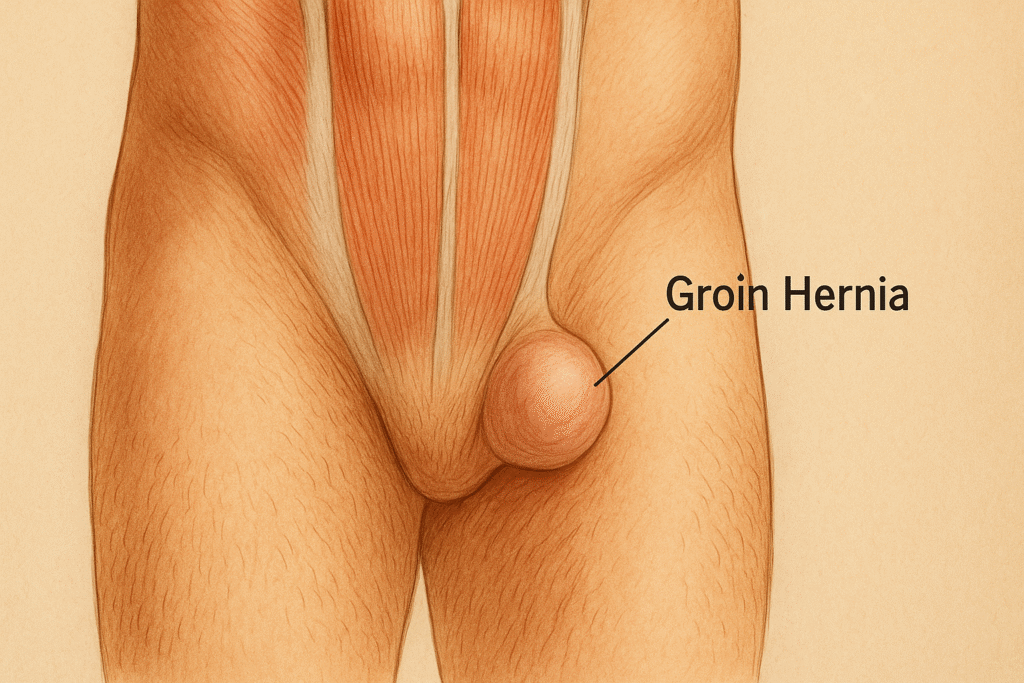
Femoral Hernias: the sneaky assassins
If inguinal hernias are rowdy and obvious, femoral hernias are discreet and deadly.
They occur below and lateral to the pubic tubercle, slipping through the femoral canal alongside vessels and lymphatics.
Why they terrify surgeons:
- Narrow neck → high risk of strangulation
- Often small and easily missed
- More common in women, especially elderly
Femoral hernias don’t negotiate. They go straight to incarceration, then to strangulation, then to emergency laparotomy if you hesitate.
As the old saying goes:
“Inguinal hernias complain; femoral hernias kill.”
Obturator Hernias: the ninjas of the hernia world
Obturator hernias are so rare that most clinicians never see one.
Which is unfortunate, because they’re also the most easily missed.
They protrude through the obturator canal, a bony tunnel carrying nerves and vessels into the thigh.
Classic patient:
- Elderly, frail, multiparous woman
- Thin (loss of preperitoneal fat uncovers the canal)
- Presents with bowel obstruction
- No visible groin lump
The clinical gem:
Howship–Romberg sign
- Pain radiating down the medial thigh
- Worse with hip extension or internal rotation
- Caused by obturator nerve compression
If you diagnose this preoperatively, treat yourself to a medal.
Risk Factors: why hernias happen
Hernias occur when pressure > strength, and anatomy provides the gap.
Pressure raisers:
- Chronic cough
- Prostatism / straining
- Heavy lifting
- Pregnancy
- Constipation
- Obesity
Strength reducers:
- Ageing tissue
- Collagen disorders
- Malnutrition
- Steroids
- Previous surgery
The groin, with its Toblerone and rings, is simply the weakest link.
Complications: when a bulge becomes a crisis
Incarceration:
Hernia contents get stuck. Pain increases: reduction fails.
Strangulation:
Blood supply is cut off. Severe pain, systemic illness, emergency surgery.
Obstruction:
If bowel is involved, vomiting and distension follow.
Hernias are benign… until they aren’t. The change can happen in hours.
Diagnosis: what the surgeon feels
Whether inguinal or femoral, the exam follows the same principles:
- Inspect (standing and lying)
- Palpate the lump
- Check cough impulse
- Test reducibility
- Identify anatomical landmarks
- Perform the deep ring occlusion test
The deep ring occlusion test:
Place your fingertip at the deep ring triangle.
Ask the patient to cough.
- If the hernia hits your fingertip → indirect
- If it hits the side of your finger → direct
- If it appears below the pubic tubercle → femoral
That single manoeuvre has passed more exams than any textbook.
Management: from trusses to mesh
Elective repair:
All symptomatic hernias deserve repair.
Modern tension-free mesh techniques dominate:
- Lichtenstein repair (open)
- TEP / TAPP repairs (laparoscopic)
Emergency repair:
Any tender, irreducible, or strangulated hernia goes straight to theatre.
Delay costs bowel.
The groin is a crossroads of pressure, anatomy, and old evolutionary mischief.
If you understand the Toblerone-shaped inguinal canal, the triangular deep and superficial rings, and the routes hernias take, the whole region suddenly makes sense.
Inguinal hernias shout.
Femoral hernias whisper.
Obturator hernias hide.
Your job is to recognise all three, ideally before the patient’s bowel pays the price.
Because in surgery, as in life, what you don’t look for, you don’t find, and what you don’t find can kill.